Before we start, if you want to help move the science forward, please subscribe for free to www.thefatemperor.com/subscribe ! That said, let’s get on with it:
Been a bit of fun lately on the old web, what with talk of native, non-damaged LDLp’s burrowing into a single-cell endothelium’s and wreaking havoc with the help of our native immune system. Well it’s an easy-to-grasp theory, I gotta hand it that. Let’s take a look at the options, shall we?
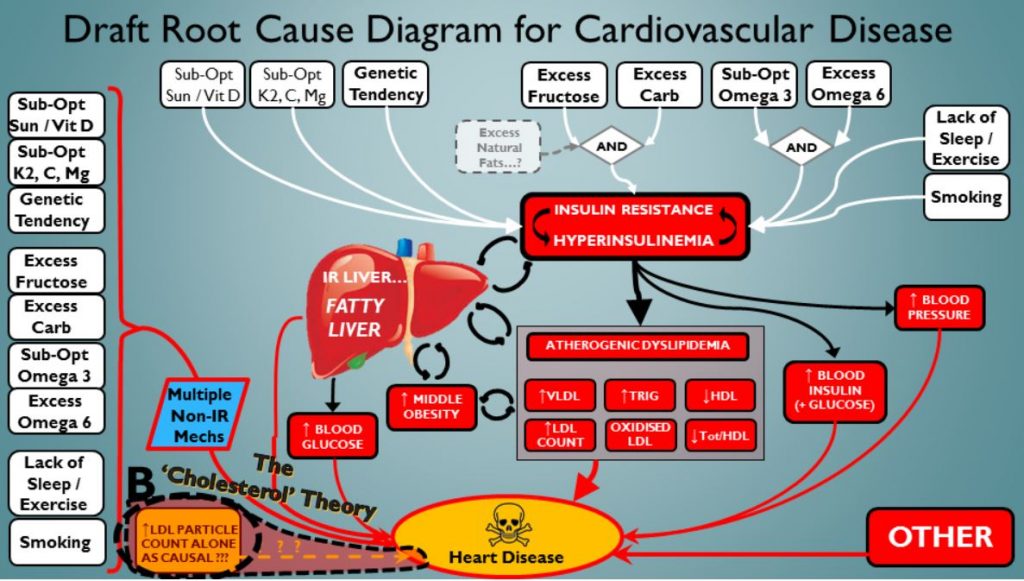
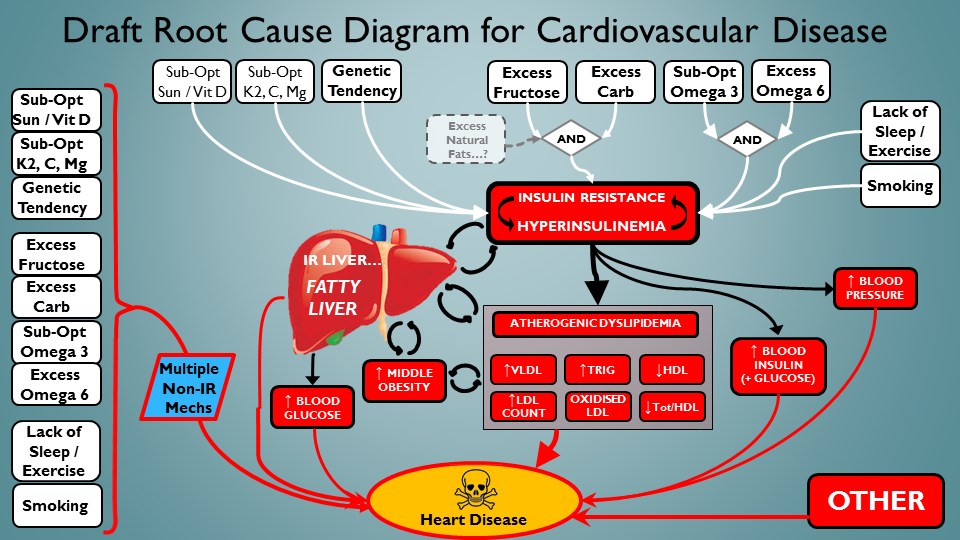
We’ll start with the established Insulin Resistance-centric driver for CVD. I haven’t included everything in this schematic, but most of the big boys are at the party:
 The common-or garden Insulin Resistance / Fatty Liver / Dyslipedemia / Met Syn Riff…
The common-or garden Insulin Resistance / Fatty Liver / Dyslipedemia / Met Syn Riff…
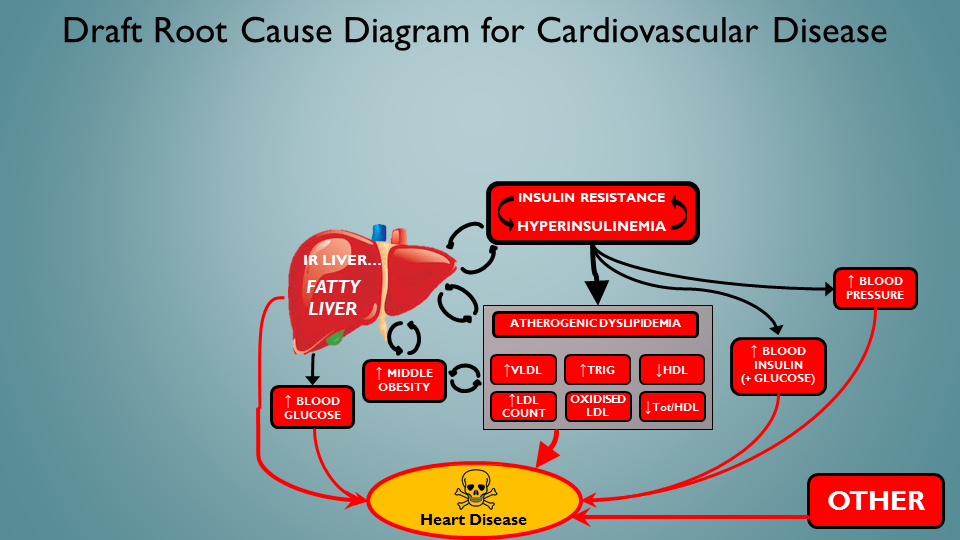
Ok, so not outrageously controversial I think, although there’s more to it. But what are the <actionable> ROOT CAUSES of this nasty, self-reinforcing destructive feedback loopery? That’s what we’d want to avoid – right? After all, we can’t replace all our internal machinery – but we can certainly maintain it optimally (for a long service life …). Let’s take a look:
 Now (in white) we see some things we can actually DO to help avoid the reaper…
Now (in white) we see some things we can actually DO to help avoid the reaper…
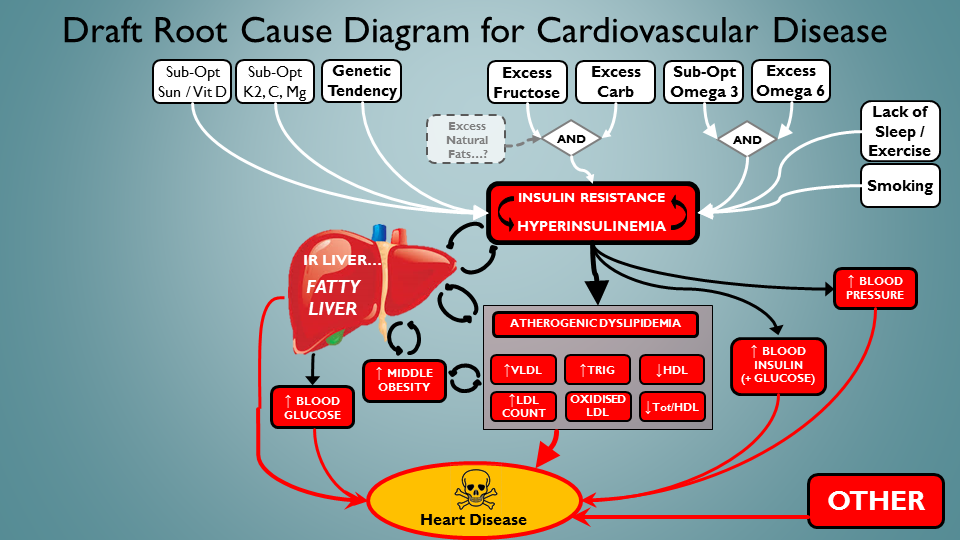
That’s a bit better. Almost feeling empowered to make a difference here. Bet if I did all those white things right, we’d see some bloods getting way better – yep, think so. But wait – this selection of addressable root causes don’t just address IR etc. In fact, this set has many connections to CVD that don’t necessarily have IR as an intermediate deleterious process. So let’s represent that here – in column of calamity down the left hand side:
 Ah, there we are. The addressable root causes do more than just the old IR riff…!
Ah, there we are. The addressable root causes do more than just the old IR riff…!
Mmmnn…still not happy. LDLp/ApoB seems kinda…underemphasised here. I mean, it’s VERY popular. We almost seem to imply here that its badness is only because it tracks with the IR / inflammatory milieu. Like…like it’s not independently toxic. Ok then – let’s give it a special seat at the root cause table. In yellow down the bottom left:
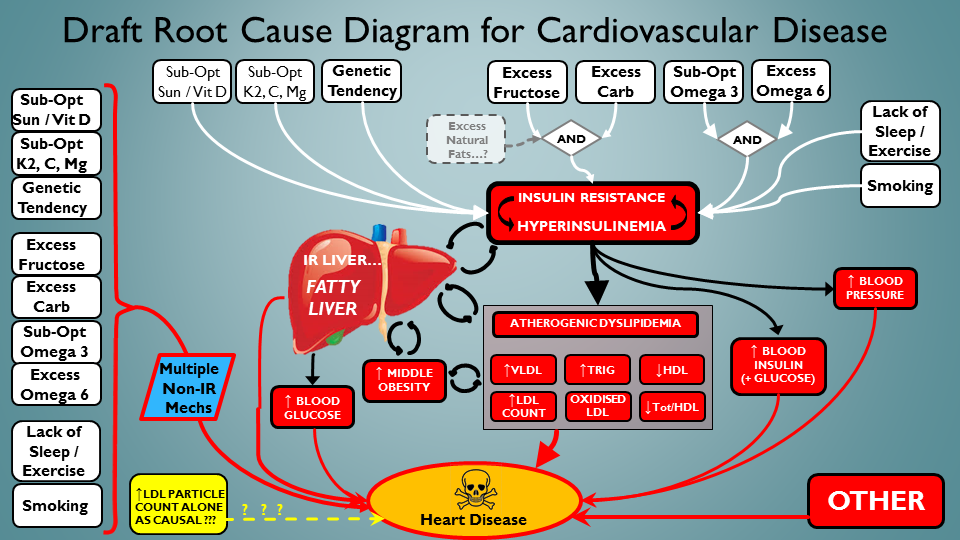 ‘Native/undamaged’ LDLp / ApoB particles get their own special root-cause-driver status ! 🙂
‘Native/undamaged’ LDLp / ApoB particles get their own special root-cause-driver status ! 🙂
Mmmnn again. I think it’s only fair to clarify the logic here though. You see, IR is a huge driver generally of high ApoB particle numbers – so the much-lauded correlation between ApoB and poor outcomes…could be mainly due to this aspect. Tricky that. Even after decades of research, I don’t think there’s any data available that tracks ApoB outcomes – specifically when all the other metrics are great. Isn’t that weird? Oh well – I guess nobody cared enough to look. So let’s break out the two routes to ApoB’s being bad. A – Through oxidative damage etc. of the particles, and the strong associations with the other root causes that drive ApoB high. And then B – through ApoB particles just being inherently toxic when there’s lots of ’em:
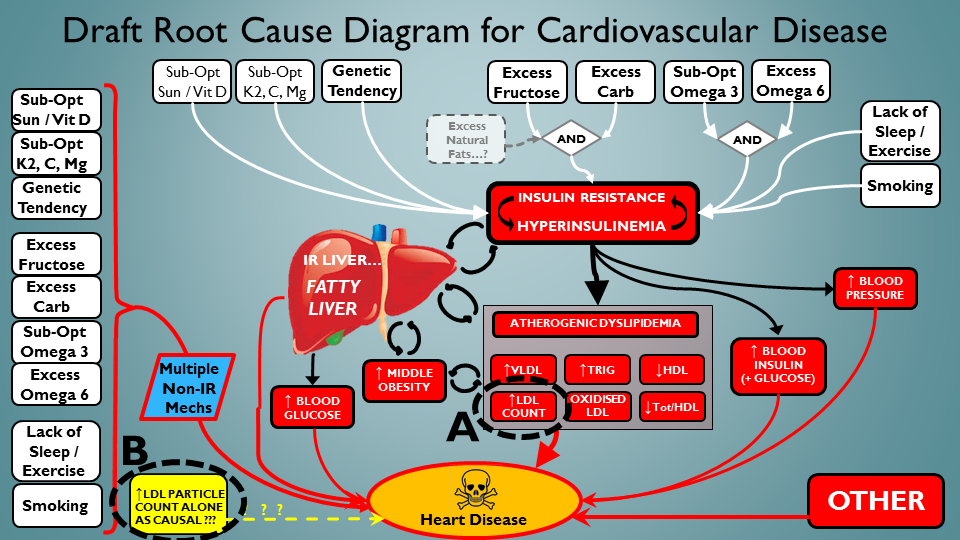 There. Separated those critters. ApoB is now a ‘Janus’ Lipoprotein !
There. Separated those critters. ApoB is now a ‘Janus’ Lipoprotein !
Just one last thing. We need to take a quick look at the relative importance of each face of ApoB particles. Let’s look a ‘A’ first – ApoB’s simply caught up as ‘substrate’ in the inflammatory milieu, partaking in the damage-fest….because many other bad things are raging throughout your system:
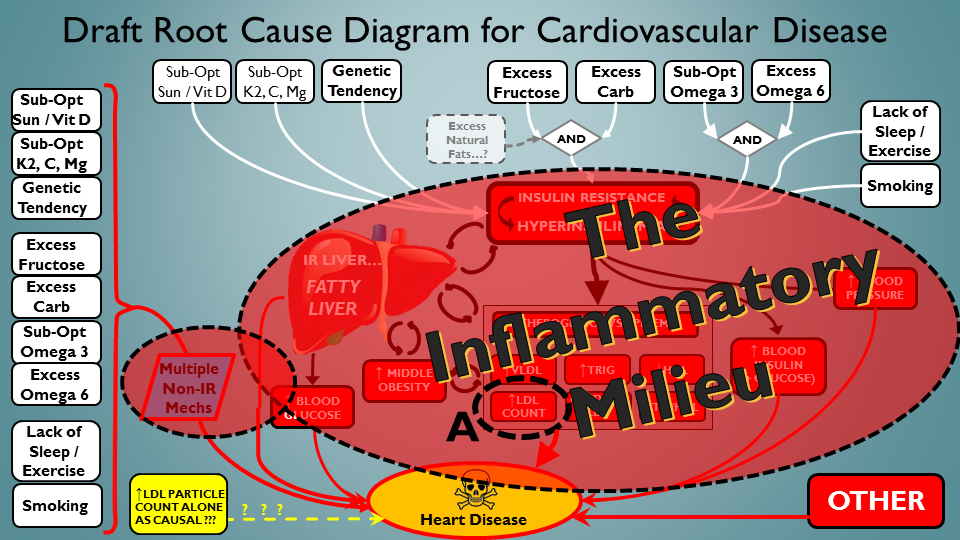 Ok, lot going on in this CVD-driving scenario – including ApoB interacting in the mess…
Ok, lot going on in this CVD-driving scenario – including ApoB interacting in the mess…
We’ll close with the other popular theory. That even without all the multifactorial mayhem of the above (or even the ‘OTHER’ drivers on the bottom right) – ApoB particles are innately, inherently, natively toxic. Mainly when there’s more of them (remember simply more of them – it’s cheating to blame ApoB if the ‘more of them’ or ‘toxicity of them’ is driven by another underlying problem). How would we depict this scenario in our final slide? Well how about this way:
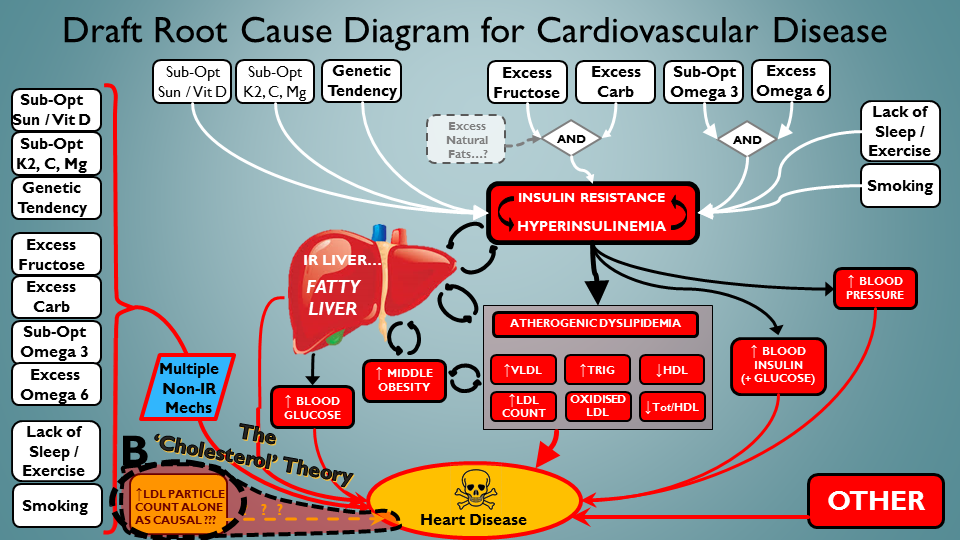 The ‘ApoB is independently toxic’ slide. That’s all folks !
The ‘ApoB is independently toxic’ slide. That’s all folks !
Well there we have it. Something seems not quite right, but I can’t put my finger on it. Maybe it’s getting my head around an evolutionarily selected physiologic component being inherently damaging? And remember, we are talking about this in the absence of something driving it to be so. If ‘X’ is driving the ApoB particles to be a problem – then ‘X’ is the root cause, not ApoB itself. We’ve just shown a big cluster of X’s in that penultimate slide.
Dr. Steve Horvitz suggested two ideas: (a) that sustained high ApoB may in turn drive IR-milieu through other paths, thus making it self a problem – but this would not simply be ‘ApoB hi is bad because it tunnels in the endo’ – still it would make ‘hi ApoB’ a cause along the top row of white elements. So lowering it for this reason could help I guess? Also (b) Receptor issues in genetic hyperlipidemia could be interactive/coupled with insulin system – hence conflating the two as cause of problems. This one I’ve mused on before, and is appealing. I’ll add another one (c) that comes to mind (again for genetic receptor issues in say FH) – if receptors screwed then ApoB gets long residence time, exposing it to deleterious modification – here again it is damage to ApoB rather then simply ‘ApoB bad because of tunneling’…
I can imagine a fusillade of irate replies, but I’ll only answer one in advance. People may say “oh but in people with genetic glitch causing super-low ApoB, there is much lower heart disease“. Quite. But ApoB is a part of the system, and stripping it right down may prevent the deleterious multiple CVD drivers from causing the usual level of damage. If you took all the fuel out of an aircraft, I dare say in a crash landing it would burn up the passengers less. But the kerosene still didn’t cause the crash. And also there are plenty of studies where ApoB doesn’t show up much – and plenty where ApoB/ApoA1 blows it away.
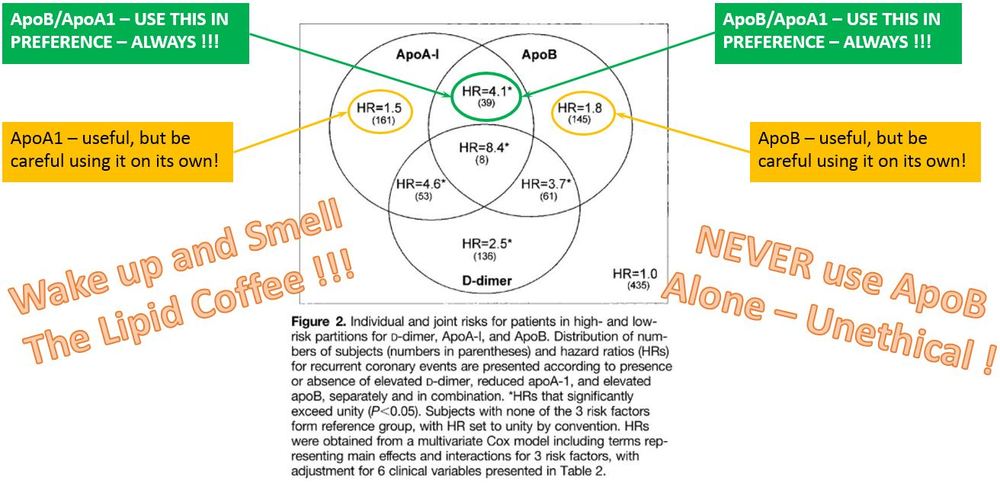
I often muse about high ApoB peeps (high risk?) whose ApoB/ApoA1 – a stronger marker – reflects low risk? Are they indeed low risk? I would say yes – go with the stronger marker. But…then their high ApoB was a very misleading marker indeed. Here is a report from Gabor Erdosi just now – consider it very CAREFULLY – consider the relative hazard ratios. Consider. Think on it before you run after ApoB willy-nilly:
Here’s another from the Women’s Health Study – on the right hand side I’ve taken out the log scale for a simpler compare – would you believe a high ApoB here (saying a person is at risk), when their ApoB/ApoA1 says the person is ok?
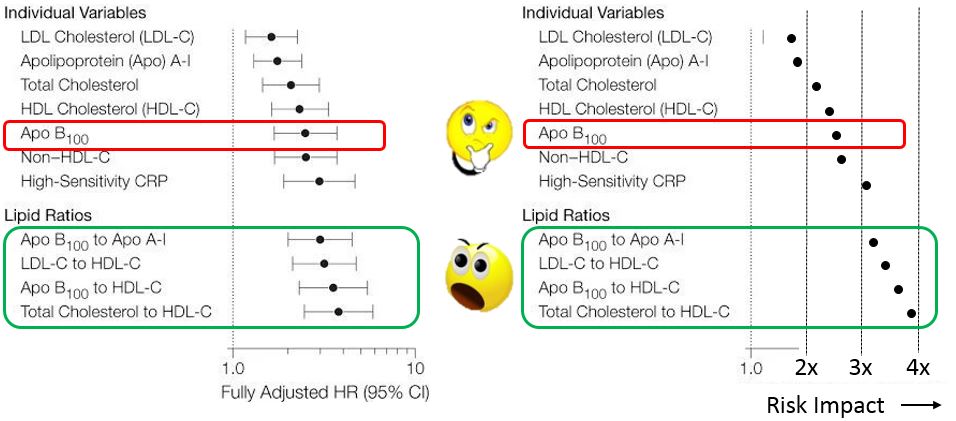 ApoB/ApoA1 encompasses so much more about the person’s physiology and risk level…
ApoB/ApoA1 encompasses so much more about the person’s physiology and risk level…
Of course, if something is causing your ApoB to be an issue, and you’re not confident you can resolve this – well then it may be the best route to lower it anyway. But the general question stands, and should be answered. It must be answered. Or we are not doing ourselves justice at all. Here’s my go-to post for those that are worried regardless – can play with ApoB levels nutritionally like Franziska did: http://www.lowcarbdietitian.com/blog/lipid-changes-on-a-very-low-carb-ketogenic-diet-my-own-experience
Great Discussion here also btw, in Peter’s post and the comments following it: http://high-fat-nutrition.blogspot.ie/2016/07/arteriosclerosis-6-and-subbotin.html
And here is the fascinating piece of detective work, with Subbotin’s paper linked at the end of this post: http://www.thefatemperor.com/blog/2016/7/3/atherosclerosis-illuminated-time-to-progress-even-the-pigs-are
p.s. the dogs in the street know that LDLc is a near-useless biomarker at this stage, so I don’t even bother including it. Still, it dominated for decades (and still dominates) the orthodox world of CVD root cause. Funny old world that, isn’t it? Wonder if ApoB turned out to be just an interacting component in CVD…would it still be seen as a primary cause…for decades more?
For more always-free content please subscribe at www.thefatemperor.com/subscribe
Also Please use the ‘share’ button below to propagate this important content…