UPDATE 9th Oct 2016: Just got this article on the debacle: https://thefatemperor.com/wp-content/uploads/2020/01/137k-Patients-Low-LDL-high-CHD-Article-UCLA.pdf
I had approximated that around 20% of these guys were on lipid-lowering medication, which didn’t change the absurdity of the result. At all. But now this article verifies it – only 21% were on the cholesterol-attacking sauce. Also LDL can drop a bit in the 24 hours or so after problems like MI occur – but these were “admission LDL’s” – blood draws taken after the guys arrived at hospital in a panic. What a farce…original blog post continues below:
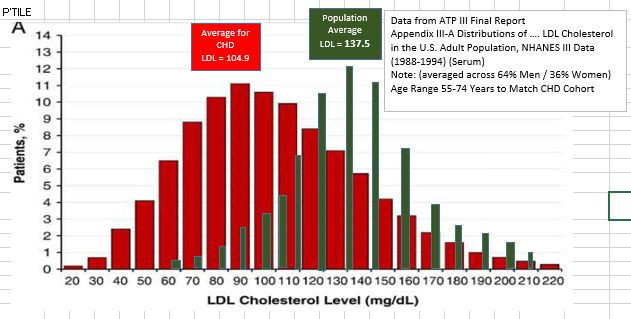
Interesting twitter chat with foremost Lipid Expert Dr. Thomas Dayspring this evening – he has acknowledged the following histograms I put together, so I feel comfortable posting them(!). Basically, the Coronary Artery Disease (CAD) Histograms (Red Bars) are from a 2009 report which measured the LDL values for >130,000 people admitted with CAD issues. I pulled the US general population LDL distribution from a similar timeframe, and averaged it to match the gender split of the CAD cohort (…Green Bars). The message is:- the majority of Myocardial Infarctions (Heart Attacks) are now driven by Insulin Resistance and excessive sugar & carbohydrate in the diet, helped by Magnesium, sunlight/D, Omega3 and other nutrient deficiencies, along with excessive Omega 6 (Note – IR with concurrent Hyperinsulinemia, not the ‘physiological IR of a low-carber). Reply from Dr. Dayspring: “Current NHANES data: majority of MI are explained by IR. But real message is unless >200 mg/dL – LDLc is terrible biomarker”. And indeed it is – LDL should never be used to diagnose, as can be seen from my graph below (Red = Coronary Disease people, Dark Green = general population).
The Coronary Disease bus is now being driven by excess sugar/carb and probably the putrid veg oils – hence the low LDL levels seen in the afflicted. Now, if you tested them for LDL-P (the particle count), you would get a slightly different story – but ‘cholesterol’ is still largely junk-science – only a problem when yer Lipoproteins are damaged…or when there are far more important underlying causes at play.
the papers: CAD patients: http://www.ahjonline.com/…/S0002-8703%2808…/fulltext and NHANES data for population: http://circ.ahajournals.org/content/106/25/3237.full
Does LDL have some predictive power when measured long in advance of the disease that drives heart attacks (i.e. the inflammatory milieu)? In spite of being a junk biomarker, it has some – that’s how it fooled them all decades ago. It depends totally on HDL value and much else though – which speaks to the core mechanisms. The following plot from Framingham illustrates:
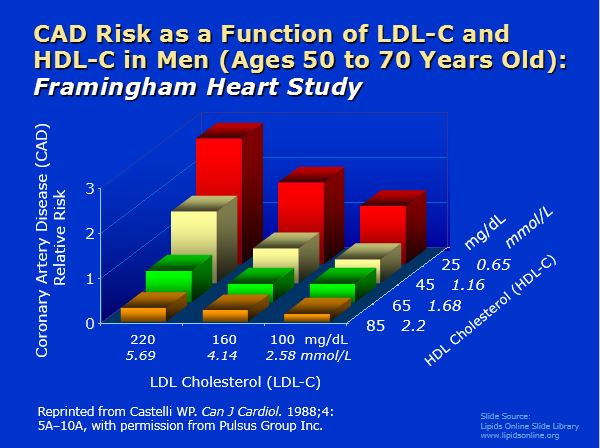
LDL is intimately interactional with HDL and other properties. Because Insulin Resistance is the primary driver of heart attacks. LDL will fool you into the ground.
LDL is just a misleading messenger…of the real deal.