Well I just hunted down a paper while researching Insulin / C-peptide as causal culprits for CHD, and this one is a zinger (all the way from 1990): http://www.ncbi.nlm.nih.gov/pubmed/8352181
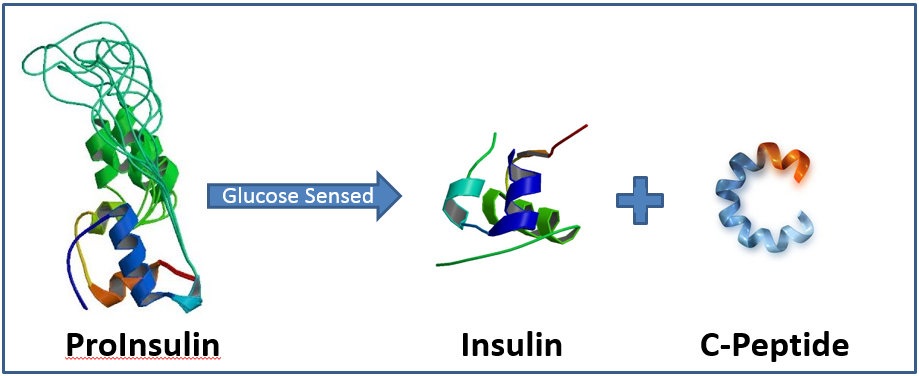
C-Peptide is important because when you provoke a molecule of insulin (i.e. carb too high, & protein somewhat – NOT fat), it comes from a pro-insulin molecule, and a C-Peptide is released also. C-Peptide doesn’t get gobbled by the liver, and it has a much longer half-life – so it could be a stronger indicator of Insulin’s nasty side – useful that.
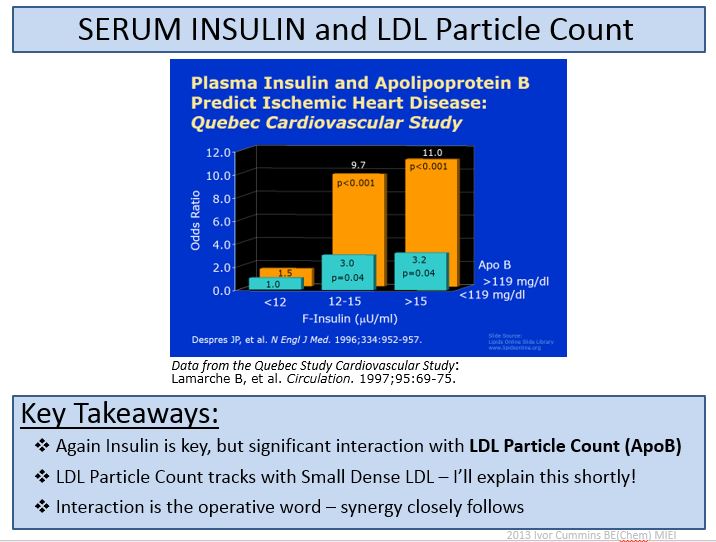
So what have we got in this paper? Well, a good kick in the arse of LDLp as a directly ‘causal’ variable in itself. Recall how it’s been said that LDL particle number is the primary driver – in that merely higher numbers of LDL’s drive the concentration gradient, that shoves them into the intima – like little grenades? I don’t fully accept it yet. Anyway, In this study we get a look at what differentiate extent of disease within an affected group: we have glucose-intolerant peeps here, and we are comparing the severe Atherosclerosis guys against the not-so-bad ones. What do we see?
Well here’s the overall variable correlations for the severe atherosclerosis versus not-so-bad in these poor peeps – note what jumps out for the severity signal. In other words, here’s what really appears to drive the extent of actual, real, inflammatory disease :
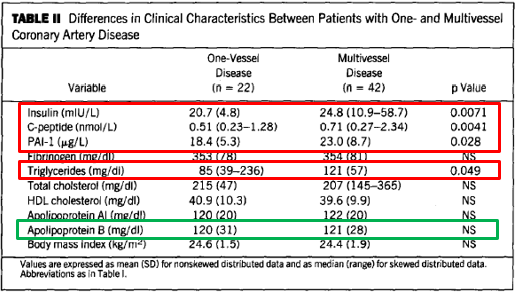
Big ooops for the LDLp theoreticians – ’cause it ain’t LDLp here. Sure, LDLp associates with atherosclerosis, because what put all these poor guys in the diseased state, tends also to drive up LDLp and down HDLc. But once the group is dysfunctional, then we get to see what really connects to the arterial damage: Insulin, C-Peptide. PAI-I. Triglyceride excess.
Let’s just remind ourselves what signified this total diseased group (less and more severe athero), showing they had done the very bold thing relative to control peeps. What variables when measured, distinguished them from the non-diseased controls. In other words, what might you see in an associational study?:
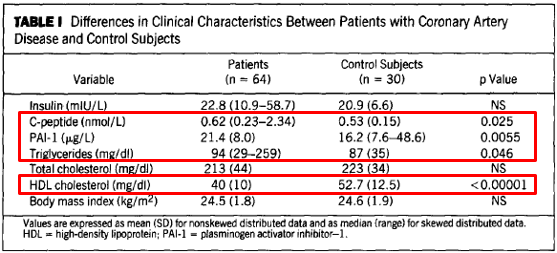
Interesting – Insulin, that we know links to the extent of disease (from from the previous ‘severity comparison’ table), now actually fails as an associational variable – possibly indicating why some associational studies are ambiguous about Insulin…it’s not a great reflection of the IR issues. HDL associates strongly, because it’s a superb biomarker for health, and indicates that you are doing the right thing – If LDLp was on this summary, of course it would associate too, indicating that you are doing the wrong thing. Yes if you have specific issues, HDL may not indicate – by all means there are myriad other causes for CVD. Trigs similarly associate, for known reasons. So one could suggest that LDLp is mainly a problem because it interacts with the inflammatory milieu via the ‘more numbers, more ingress’ play – and most of all, it interacts with Insulin issues. Old chestnut again below?