Great panel discussion at Low Carb Breckenridge. Here Mike Eades clarifies an important note around the CAC score. While it is the most powerful test for cardiac and all-cause mortality prediction (by a mile), there are some nuances.
Specifically the Volume component of the CAC score is important to scrutinize (the CAC score has both a Density and a Volume component). If you have a high score where Density dominates over Volume, your risk may be ok. If your score advances over the years, dominated by density (with volume falling) – you do not have appreciable risk. The worst case is where Volume dominates over Density – this is a major flag for unstable plaque presence.
The paper Mike notified me of some time back, is very revealing in this context:
LINK: Eades Calcium Density of Coronary Artery Plaque and Risk of Incident Cardiovascular Events-1
See The Widowmaker Movie (2015) here – a fascinating docu-drama showing where the cardiovascular world went so disasterously wrong ! https://www.youtube.com/watch?v=NSPcuGjstN4&feature=youtu.be&t=108s
In the following clip, Mike explains the nuance most eloquently! Discussion in more detail at end of this post
The power of CAC illustrated in one of my earlier posts – click the image below to gain the insights! :

The Widowmaker Movie – click below to watch for a dollar 🙂

This arena is nuanced indeed. You do divide the Overall score by the (volume/2.5) to get the density number, but it is a tricky one e.g.:
– If your Agatston value is very low, even with low density quotient – you are in ok shape – but only because these low density guys are “Low overall score” guys (they have little plaque, and it ain’t too calcified – but they have little burden anyway so ok).
– If your density value is high you may also be in ok shape – these high density guys have high overall scores, but are protected by their relative density – lots of plaque, but nicely consolidated with Ca – nature is working well for them.
– the problem guys are the ones with high score and high volume – these have high plaque burden and it is not stabilized adequately by nice dense calcification !
The secret is buried in this table:
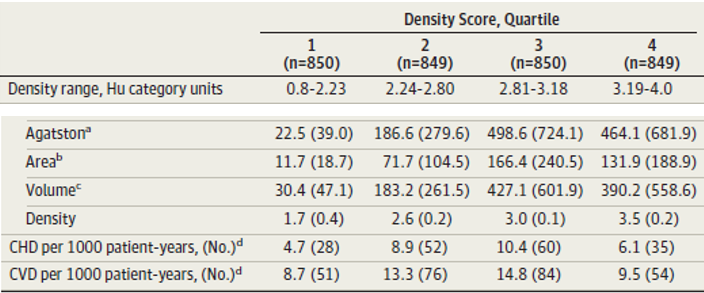
Someone with a high overall score, but high in density – is at similar risk to the average guy who has a CAC score of around 20. See above on the “density” line – the guys with high CAC (Agatston) scores in right hand column have an average density of ~3.5 and their risk thus begins to sharply fall off, making them like Agatston=20 scorers.
It’s a tricky one for sure, kind of a hyperbolic relationship with two vectors involved – overall score versus density quotient.
AND NOW THE PLUMBING ANALOGY:
Explained it to my daughter who is going for medicine in college. Imagine buildings with corroding pipes:
1. Some buildings have small pockets of corrosion, but it is not really patched up much by the plumbers – they have lowish risk of flooding. (low CAC score, low volume score, low density peeps).
2. Then there are buildings with a lot of corrosion all over the system – but great plumbers have patched up all the weak areas (high CAC score, low volume score, high density peeps).
3. Then there are the shitty buildings – they have lots of corrosion all over, but crap plumbers who have not patched up very well (high CAC score, high volume, low density peeps). The latter need to get good plumbers in fast….or to go #LCHF asap !!!!
(p.s. the last guys (3) are generally poorly-controlled diabetics – corroding fast before their tattered systems can shore up the damage)